Reduced biventricular contractility during exercise in adults with small, unrepaired ventricular septal defects: an echocardiographic study.
Maagaard M, Heiberg J, Redington AN, Hjortdal VE.
Eur J Cardiothorac Surg. 2020 Mar 1;57(3):574-580. doi: 10.1093/ejcts/ezz278.
PMID: 31625565
Select item 31972544
Take Home Points:
- Patients with small, unrepaired ventricular septal defect (VSD) who are apparently well, do have physiological impairment.
- A reduction in systolic and isovolumetric acceleration and isovolumetric velocity at the left and right ventricular free wall and septum at rest and during exercise were noted in patients with small VSD compared to controls.
- The left ventricular isovolumetric acceleration is inversely correlated to the size of the shunt.

Commentary from Dr. M.C. Leong (Kuala Lumpur, Indonesia), section editor of ACHD Journal Watch: Patients with a small ventricular septal defect (VSD) and non-significant shunt were often perceived to be healthy. These small VSD were seen to be haemodynamically insignificant and hence do not bring any damage to health apart from the slight but negligible increase in the risk for infective endocarditis. However, recent studies have demonstrated their effect in limiting patient’s functional capacity. This study aimed to assess the effect of small, haemodynamic insignificant VSD’s on the cardiac contractility especially during exercise. Cardiac contractility was assessed via isovolumetric acceleration, a sensitive echocardiographic marker of cardiac contractility which is independent of the loading condition of the ventricles.
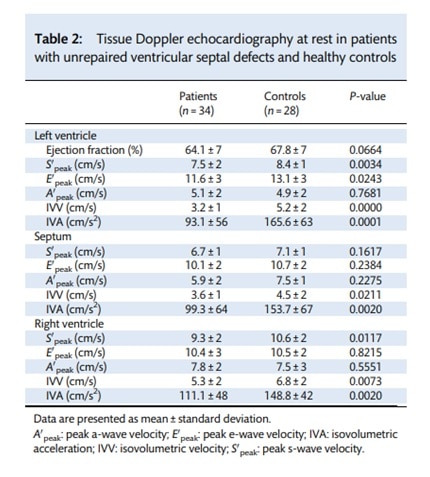 This is a case control study, involving 34 patients with insignificant VSD shunts (median shunt ratio on cardiac magnetic resonance flow assessment: 1.2) and 28 healthy individuals. At baseline, the two groups were found to be comparable in terms of age, body weight, heart rate and blood pressures. At rest, patients with small VSD’s were noted to have a lower isovolumetric acceleration (IVA) and isovolumetric velocity (IVV) at the left and right ventricular free wall as well as the septal wall (Table 2).
This is a case control study, involving 34 patients with insignificant VSD shunts (median shunt ratio on cardiac magnetic resonance flow assessment: 1.2) and 28 healthy individuals. At baseline, the two groups were found to be comparable in terms of age, body weight, heart rate and blood pressures. At rest, patients with small VSD’s were noted to have a lower isovolumetric acceleration (IVA) and isovolumetric velocity (IVV) at the left and right ventricular free wall as well as the septal wall (Table 2).
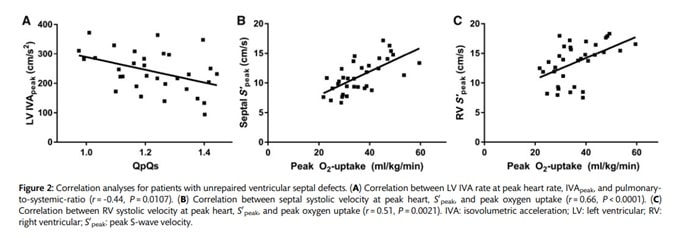
During exercise, patients with small VSD’s demonstrated a lower IVA, IVV and peak systolic velocity at the left and right ventricular free wall and septum compared to controls (Figure 1). On further analysis, left ventricular IVA was noted to be inversely correlated to the shunt size. Peak exercise capacity was positively correlated with right ventricular IVV and septal IVV but not the left ventricular IVV (Figure 2).

This study, albeit being a small one, provides insights to the non-benign nature of small, haemodynamically insignificant VSDs. The effect of small VSDs on cardiac contractility is present not only at rest but also during exercise. However, these findings have yet to translate into a recommendation for closure as a different study by the same group of authors showed lower peak systolic velocity and IVA in patients post VSD closure compared to controls during exercise (ref). This study showed that even after closure of the VSD, there was impairment of the ventricular contractility during exercise which suggests that the ventricular contractility does not improve with VSD closure. Long term outcome of these group of patients with small VSDs compared to normal controls would be interesting to note.